Ramathibodi Lung Cancer Consortium Model
ศูนย์ความเป็นเลิศด้านโรคมะเร็ง คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล



{:th}
Ramathibodi Lung Cancer Consortium Model
ศูนย์ความเป็นเลิศด้านโรคมะเร็ง คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล
ผลงานวิจัย :
Ramathibodi Lung Cancer Consortium Model
ผู้วิจัย :
ผศ.พญ.ธัญนันท์ เรืองเวทย์วัฒนา (หัวหน้าโครงการ)
Ramathibodi Lung Cancer Consortium (RLC) 34 ท่าน (รวมที่ปรึกษา และแพทย์ทุกสาขาที่เกี่ยวกับการรักษาโรคมะเร็งปอด แพทย์ผ่าตัด แพทย์รังสีรักษา รังสีวินิจฉัย นิวเคลียร์ แพทย์อายุรศาสตร์มะเร็ง แพทย์โรคปอด แพทย์พยาธิ แพทย์ X – Ray Intervention พยาบาล เภสัชกร และเจ้าหน้าที่ใน RLC)
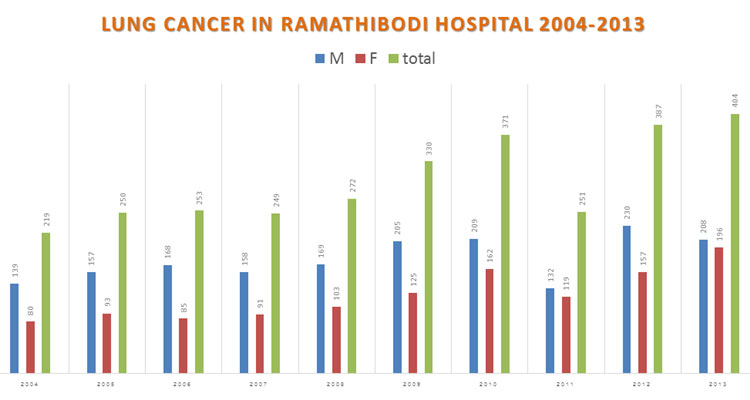
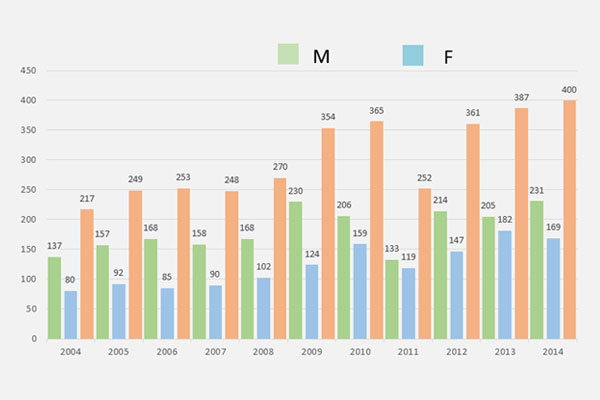
เนื่องจากโรคมะเร็งปอด เป็นโรคที่เป็นปัญหาสำคัญของทุกประเทศทั่วโลก ในปี พ.ศ. 2555 ผู้ป่วยมะเร็งปอดรายใหม่ทั่วโลกอยู่ที่ 1.8 ล้านคน และมีอัตราตายอยู่ที่ 1.6 ล้านคน มีอัตราการรอดชีวิตที่ 5 ปี อยู่ที่ 17.8% ซึ่งต่ำกว่ามะเร็งชนิดอื่นที่พบบ่อย เช่น มะเร็งต่อมลูกหมาก 99.6%, มะเร็งเต้านม 90.5%, และ มะเร็งลำไส้ 65.4 ข้อมูลจากสถาบันมะเร็งในประเทศไทย ในปี พ.ศ. 2555 พบว่ามีผู้ป่วยรายใหม่ที่เป็นมะเร็งปอดสูงเป็นอันดับที่ 2 ในเพศชาย และเป็นลำดับที่ 4 ในเพศหญิง ซึ่งสอดคล้องกับข้อมูลโรงพยาบาลรามาธิบดี (Ramathibodi Cancer Registry) จากข้อมูลดังกล่าวจะเห็นว่า โรคมะเร็งปอดเป็นโรคที่มีอุบัติการณ์ และอัตราตายที่สูงทั่วโลก ข้อมูลในโรงพยาบาลรามาธิบดี ปี พ.ศ. 2547 – 2556 ดังแสดงในภาพที่ 1 พบว่า ผู้ป่วยใหม่ที่ได้รับการวินิจฉัยว่าเป็นโรคมะเร็งปอด ที่มารักษาที่โรงพยาบาลรามาธิบดี มีจำนวนมากขึ้นเรื่อย ๆ ทุกปี ทั้งเพศชาย และเพศหญิง ล่าสุดปี 2556 นั้นมีผู้ป่วยใหม่ 404 รายต่อปี
ในปัจจุบัน การสืบค้น และการรักษาโรคมะเร็งปอดมีความก้าวหน้าไปอย่างมาก มีการตรวจค้นลงถึงระดับพันธุศาสตร์ โดยศึกษาถึงการเปลี่ยนแปลงของยีนกลายพันธุ์เมื่อเกิดโรคมะเร็งปอด เพื่อที่จะให้การรักษาที่เฉพาะเจาะจงมากขึ้น ทำให้มีค่าใช้จ่ายที่เกิดจากการตรวจ และการรักษามากขึ้นเช่นกัน จากการที่ผู้ป่วยมะเร็งปอดมีจำนวนมากขึ้น และมีการสืบค้นหลายขั้นตอนก่อนที่จะรักษา เพื่อให้ได้มาซึ่งการวินิจฉัยโรคที่ถูกต้องครบถ้วน ทั้งชนิดของเซลล์มะเร็ง ชนิดของยีนกลายพันธุ์ ระยะของโรค รวมทั้งการประเมินขั้นตอน และวิธีการรักษา ซึ่งประกอบด้วย การผ่าตัด การฉายแสง การให้ยาเคมีบำบัด และการให้ยาต้านเฉพาะจุด ซึ่งจะเริ่มการรักษาด้วยวิธีใดนั้น ขึ้นอยู่กับหลายปัจจัยดังกล่าวข้างต้น รวมถึงสภาวะร่างกายและจิตใจของผู้ป่วยก่อนเริ่มการรักษา ดังนั้น ผู้ป่วยจะต้องพบหมอหลายแผนก และต้องมาโรงพยาบาลหลายครั้งก่อนจะเริ่มการรักษา และการทำการประเมินตัวโรคต่าง ๆ รวมถึงการตัดสินใจในการรักษา โดยส่วนใหญ่ต้องใช้การตัดสินใจร่วมกันของแพทย์แผนกต่าง ๆ เช่น แพทย์อายุรกรรมมะเร็งวิทยา แพทย์โรคปอด แพทย์รังสีรักษาและรังสีวินิจฉัย แพทย์นิวเคลียร์ แพทย์พยาธิวิทยา ที่จะต้องประเมินและดูผู้ป่วยร่วมกัน อีกทั้งในขณะทำการรักษาก็ต้องอาศัยทีมเภสัชกร ทีมพยาบาล และทีม Palliative Care ในการดูแลผู้ป่วยโรคมะเร็งปอดอีกด้วย
จากปัญหาทั้งหมดดังกล่าว ทำให้เกิดแนวความคิดการจัดตั้งกลุ่มงานดูแลรักษาผู้ป่วยโรคมะเร็งปอด (Ramathibodi Lung Cancer Consortium: RLC) ซึ่งวัตถุประสงค์ก็เพื่อที่จะดูแลคนไข้มะเร็งปอดแบบครบวงจร มีการตรวจวินิจฉัยและรักษาแบบ ONE – STOP – SERVICE โดยมีผู้ป่วยเป็นศูนย์กลางของการรักษา แพทย์ทุกแขนงที่เกี่ยวข้องกับการรักษาโรคมะเร็งปอดดูคนไข้ร่วมกัน และตัดสินใจการรักษาร่วมกัน เพื่อให้ผู้ป่วยโรคมะเร็งปอดได้เข้าถึงการตรวจวินิจฉัยและการรักษาโดยเร็วขึ้น และลดจำนวนครั้งของการมาโรงพยาบาลลงในช่วงที่กำลังประเมินและวินิจฉัยโรคก่อนเริ่มการรักษา นอกจากนี้กลุ่ม RLC ยังได้มีการร่วมมือกันให้ความรู้เกี่ยวกับโรคมะเร็งปอดกับบุคลากรทุกแขนง Residents และ Fellows ของทุกแผนก และยังมีการวิจัยเกี่ยวกับมะเร็งปอดร่วมกันอย่างต่อเนื่องอีกด้วย
RLC นั้น ได้จัดตั้งและมีการประชุมของแพทย์ทุกสาขา พยาบาล เภสัชกร ที่เกี่ยวข้องกับการดูแลรักษาผู้ป่วยโรคมะเร็งปอด (Multidisciplinary Team) ทุกวันอังคารสัปดาห์ที่ 1 และ 3 ของเดือน เพื่อดูแลประเมินผู้ป่วยมะเร็งปอดที่ต้องการการดูแลแบบสหสาขาร่วมกัน เพื่อให้ผู้ป่วยได้เข้าถึงการตรวจวินิจฉัย และการรักษาได้รวดเร็วที่สุด ถ้ามีวันอังคารสัปดาห์ที่ 5 เป็นบางเดือนก็จะมีการประชุมคณะกรรมการ RLC เพื่อหาแนวทางแก้ปัญหาต่าง ๆ ในการดำเนินงานร่วมกัน และรวมกลุ่มกันทำวิจัย รวมทั้ง Update ความรู้ใหม่ ๆ ทางวิชาการในแต่ละแขนงร่วมกันอีกด้วย โดย RLC ได้เริ่มดำเนินงานครั้งแรกวันที่ 7 ตุลาคม พ.ศ. 2557
ซึ่งนับถึงขณะที่ทำการวิเคราะห์ข้อมูลโครงการนี้ เป็นเวลา 2 ปี 7 เดือน RLC ได้มีการดำเนินงานมาอย่างต่อเนื่อง โดยได้นำผู้ป่วยเข้ามาประชุมปรึกษาหารือร่วมกันทั้งหมด 236 ราย มีบางรายที่นำมาเข้าซ้ำเพื่อติดตามผลการรักษากัน มีการจัดให้ความรู้ร่วมกัน Lecture 15 ครั้ง รวมถึงมีการประชุมคณะกรรมการ RLC กันทั้งหมด 12 ครั้ง ขณะนี้โครงการนี้จึงได้มีการวิเคราะห์ผล ตัวชี้วัดต่าง ๆ ที่แสดงถึงคุณภาพ และความรวดเร็วในเข้าถึงการบริการ และการรักษาของผู้ป่วยโรคมะเร็งปอดในโรงพยาบาลรามาธิบดี โดยผ่าน Ramathibodi Lung Cancer Consortium Model โดยเปรียบเทียบกับการดำเนินการรักษาผู้ป่วยโรคมะเร็งปอดก่อนที่จะมีการจัดตั้ง RLC ขึ้น
เป้าหมาย :
1.) เพื่อพัฒนาคุณภาพการบริการ ความรวดเร็ว ในการเข้าถึงการตรวจและการรักษาในผู้ป่วยโรคมะเร็งปอดในโรงพยาบาลรามาธิบดี โดยผ่าน Ramathibodi Lung Cancer Consortium Model ซึ่งจะทำให้รวดเร็วขึ้น และทำให้ผลการรักษาดีขึ้น
2.) เพื่อรวมตัวกันพัฒนาการวิจัยในผู้ป่วยโรคมะเร็งปอด
3.) เพื่อพัฒนา และ Update ความรู้ในสาขาวิชาต่าง ๆ ที่เกี่ยวข้องกับมะเร็งปอดอย่างต่อเนื่อง และให้ความรู้แก่บุคลากรทุกแขนง รวมทั้งแพทย์ประจำบ้าน และแพทย์ประจำบ้านต่อยอด และขยายไปถึงการให้ความรู้ประชาชน ผู้ป่วย และญาติผู้ป่วย
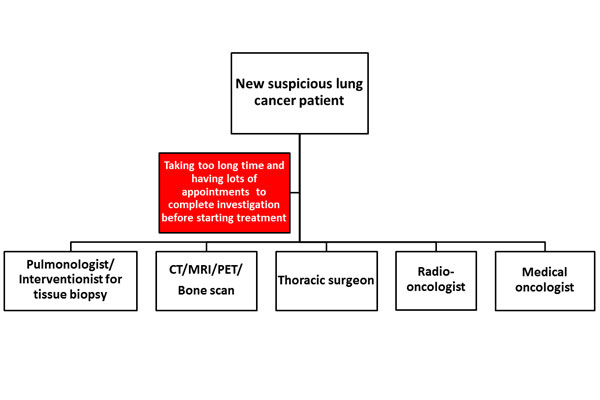
ปัญหาและสาเหตุ โดยย่อ : ผู้ป่วยใหม่ที่สงสัยว่าเป็นโรคมะเร็งปอด จะต้องพบหมอหลายแผนก และต้องมาโรงพยาบาลหลายครั้ง เพื่อประเมินตัวโรค และวินิจฉัยโรค ก่อนจะเริ่มการรักษา
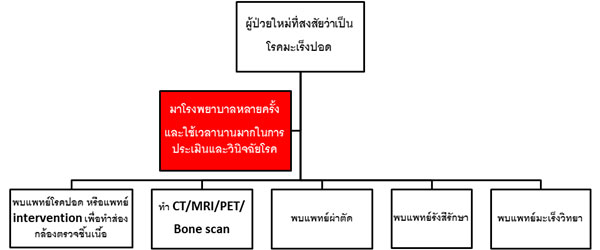
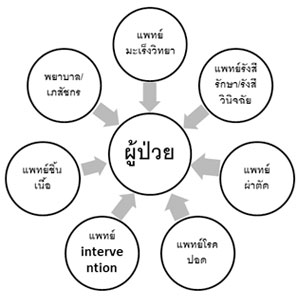
จาก Workflow ดังภาพที่ 2 พบว่า ผู้ป่วยต้องมีการประเมินตัวโรค เพื่อการวินิจฉัยโรค โดยต้องเดินทางมาโรงพยาบาลพบแพทย์หลายสาขาหลายครั้ง รวมทั้งต้องมีการทำ Imaging Study ต่าง ๆ การตรวจชิ้นเนื้อ ทำให้ใช้เวลานานมากกว่าที่จะได้รับการประเมิน และการวินิจฉัยโรคอย่างถูกต้อง ทำให้การรักษาโรคเริ่มได้ช้า ซึ่งอาจจะส่งผลทำให้ผลการรักษาไม่ดี หรือผู้ป่วยมีอาการทรุดหนักไปก่อนเริ่มการรักษา และโดยส่วนใหญ่โรคมะเร็งปอด เป็นโรคที่ต้องใช้การตัดสินใจร่วมกันของแพทย์สหสาขา รวมถึงการทบทวน Scan ต่าง ๆ และ ผลทางชิ้นเนื้อต่าง ๆ ซึ่งต้องอาศัยความรู้ความชำนาญของผู้เชี่ยวชาญหลายแขนง จึงทำให้เกิดแนวความคิดการจัดตั้งกลุ่มงานดูแลผู้ป่วยโรคมะเร็งปอด ซึ่งวัตถุประสงค์ก็เพื่อที่จะดูแลคนไข้มะเร็งปอดแบบครบวงจร มีการตรวจวินิจฉัยและรักษาแบบ ONE – STOP – SERVICE ซึ่งเน้นแบบ PATIENT – CENTER CARE SYSTEM โดยแพทย์ทุกแขนงที่เกี่ยวข้องกับการรักษาโรคมะเร็งปอด ดูคนไข้ร่วมกัน โดยใช้ผู้ป่วยเป็นศูนย์กลาง และตัดสินใจการรักษาร่วมกัน เพื่อให้ผู้ป่วยโรคมะเร็งปอดได้เข้าถึงการตรวจวินิจฉัย และการรักษาโดยเร็วขึ้น และลดจำนวนครั้งของการมาโรงพยาบาลลงในช่วงที่กำลังประเมินและวินิจฉัยโรคก่อนเริ่มการรักษา ดังแสดงดัง Workflow ภาพที่ 3 และมีการติดตามผู้ป่วยว่าได้รับการนัดหมายต่าง ๆ อย่างรวดเร็ว และได้รับการรักษาเป็นไปตามที่ได้เข้าร่วมประชุมดูผู้ป่วยร่วมกันหรือไม่ ซึ่งวิธีนี้จะทำให้คุณภาพ และความรวดเร็วในเข้าถึงการบริการ และการรักษาของผู้ป่วยโรคมะเร็งปอดในโรงพยาบาลรามาธิบดี โดยผ่าน Ramathibodi Lung Cancer Consortium Model รวดเร็วขึ้นทำให้ผลการรักษาดีขึ้นอีกด้วย
กิจกรรมการพัฒนา :
ตารางที่ 1 : แสดงกิจกรรมการดำเนินการต่าง ๆ ของ RLC
| กิจกรรม | ระยะเวลาดำเนินการ (เดือน/ปี) | ผู้รับผิดชอบ/บทบาทหน้าที่ของผู้รับผิดชอบ | |||
| ปีที่ 1 | ปีที่ 2 | ปีที่ 3 | ต่อเนื่อง | ||
| 1.) จัดตั้งกลุ่ม RLC ขึ้น เมื่อวันที่ 7 ต.ค. 2557 | ผศ.พญ.ธัญนันท์ เรืองเวทย์วัฒนา อ.นพ. วิรัช ตั้งสุจริตวิจิตร |
||||
| 2.) มีการเริ่มประชุม RLC Tumor Board เพื่อดูผู้ป่วยร่วมกัน ตั้งแต่วันที่ 7 ต.ค. 2557 โดยจัดทำทุกวันอังคาร สัปดาห์ที่ 1 และ 3 ของเดือน |
กลุ่ม RLC | ||||
| 3.) มีการประชุมคณะกรรมการ RLC ทุกวันอังคาร สัปดาห์ที่ 5 ของเดือน | กลุ่ม RLC | ||||
| 4.) มีการจัด Lecture เพื่อ Update บุคลากรทุกแขนง | กลุ่ม RLC | ||||
| 5.) มีการทำวิจัยร่วมกัน | กลุ่ม RLC | ||||
| 6.) มีการจัดประชุมวิชาการโรคมะเร็งปอด | กลุ่ม RLC | ||||
RLC ได้เริ่มดำเนินงานครั้งแรก วันที่ 7 ตุลาคม พ.ศ. 2557 ซึ่งนับถึงขณะที่มีการวิเคราะห์ข้อมูล เป็นเวลา 2 ปี 7 เดือน ได้มีการดำเนินงานมาอย่างต่อเนื่อง โดยได้นำผู้ป่วยเข้ามาประชุมปรึกษาหารือ ร่วมกันทั้งหมด 236 ราย มีบางรายที่นำมาเข้าซ้ำเพื่อติดตามผลการรักษากัน มีการจัดให้ความรู้ร่วมกัน Lecture 15 ครั้ง รวมถึงมีการประชุมคณะกรรมการ RLC กันทั้งหมด 12 ครั้ง ขณะนี้โครงการนี้จึงได้มีการเก็บข้อมูลและวิเคราะห์ผล ตัวชี้วัดต่าง ๆ ที่แสดงถึงคุณภาพ และความรวดเร็วในเข้าถึงการบริการ และการรักษาของผู้ป่วยโรคมะเร็งปอดในโรงพยาบาลรามาธิบดี โดยผ่าน Ramathibodi Lung Cancer Consortium Model (จำนวนผู้ป่วยกลุ่ม RLC = 200 ราย) โดยเปรียบเทียบกับการดำเนินการรักษาผู้ป่วยโรคมะเร็งปอดก่อนที่จะมีการจัดตั้ง RLC ขึ้น (จำนวนผู้ป่วยกลุ่ม Control = 81 ราย)
การประเมินผลการเปลี่ยนแปลง :
จากผลการเก็บและวิเคราะห์ข้อมูลทั้งหมด ตั้งแต่มีการจัดตั้งกลุ่ม RLC (2 ปี 7 เดือน) พบว่า Multidisciplinary Team รวมทั้งการรักษาแบบ ONE – STOP – SERVICE โดยมีผู้ป่วยเป็นศูนย์กลาง โดยมีแพทย์ทุกแขนงมาดูผู้ป่วยร่วมกัน ตัดสินใจรักษาร่วมกัน โดยผ่าน Ramathibodi Lung Cancer Consortium Model ทำให้สามารถพัฒนาคุณภาพการบริการ การตรวจ การวินิจฉัยโรค และการรักษาโรค ได้ดีขึ้นอย่างมีนัยสำคัญทางสถิติ เมื่อเทียบกับการตรวจรักษาก่อนมีการจัดตั้ง RLC ในทุกตัวชี้วัด ดังแสดงใน ตารางที่ 2 และ 3 ไม่ว่าจะเป็นระยะเวลาการเข้าถึงการรักษาต่าง ๆ ทั้งการให้ยาเคมีบำบัด การผ่าตัด การให้รังสีรักษา รวมถึงระยะเวลาในการเข้าถึงการตรวจต่าง ๆ เช่น การทำ Imaging Study ต่าง ๆ การทำการตรวจชิ้นเนื้อ ทั้งจากการส่องกล้องหลอดลม และการทำ Transthoracic Biopsy ระยะเวลาต่าง ๆ เหล่านี้ ลดลงอย่างมีนัยสำคัญทางสถิติ และจำนวนครั้งการมาโรงพยาบาลก็ลดลงอย่างมีนัยสำคัญทางสถิติ เมื่อเปรียบเทียบกับก่อนตรวจรักษาก่อนมีการจัดตั้งกลุ่ม RLC
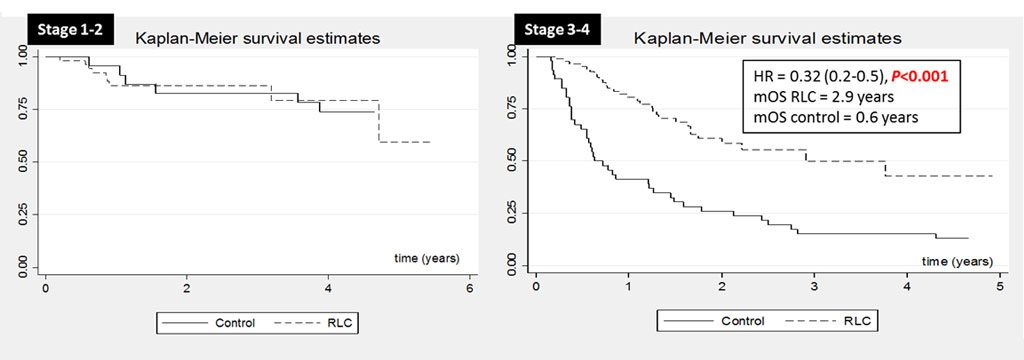
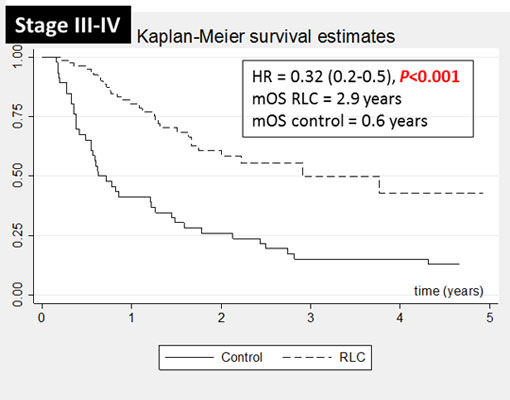
และนอกจากนี้ เมื่อนำมาวิเคราะห์ผลเพิ่มเติมถึงอัตราการอยู่รอดชีวิตของผู้ป่วยมะเร็งปอดที่ผ่าน RLC โมเดล พบว่าผู้ป่วยมีอัตราการอยู่รอดชีวิตที่ยืนยาวขึ้นอย่างมีนัยสำคัญทางสถิติ เมื่อเปรียบเทียบกับผู้ป่วยมะเร็งปอดที่ไม่ได้ผ่าน RLC โมเดล หรือผู้ป่วยมะเร็งปอดก่อนมีการจัดตั้ง RLC ดังแสดงในตารางที่ 4 และเมื่อแยกผู้ป่วยตามระยะของโรคคือ ระยะแรกเริ่ม (Stage 1 – 2 : ระยะที่รักษาหายจากการผ่าตัดเป็นหลัก) และระยะที่เป็นมากหรือระยะลุกลาม (Stage 3 – 4) ก็พบว่าผู้ป่วยมะเร็งปอดที่มีระยะของโรคเป็นระยะ 3 – 4 นั้น ถ้าผ่านกลไกการทำงานของ RLC โมเดล จะมี Overall Survival (OS) หรือความยืนยาวของชีวิตที่มากกว่าผู้ป่วยที่ไม่ได้ผ่าน RLC อย่างมีนัยสำคัญทางสถิติ ดังแสดงในภาพที่ 6 ส่วนในระยะแรกเริ่มนั้นขณะนี้ OS ยังไม่ต่างกันระหว่างสองกลุ่ม เนื่องจากเป็นระยะที่อัตราการรอดชีวิตสูงอยู่แล้ว และขณะนี้ระยะเวลาในการติดตามยังไม่มากพอ
ตารางที่ 2 : แสดงตัวชี้วัดผลสำเร็จหลัก ผลดำเนินโครงการ เปรียบเทียบระหว่างก่อนและหลังมีการจัดตั้ง RLC
| ตัวชี้วัด | เป้าหมาย | ผลดำเนินการ | ||
| ก่อนจัดตั้ง RLC (Control) N = 81 |
หลังจัดตั้ง RLC N = 200 |
P – value | ||
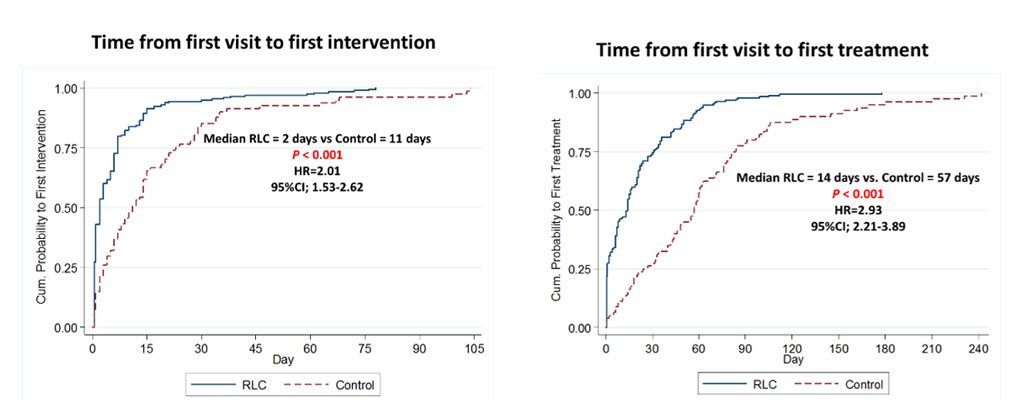
| Time from First Visit to First Intervention (Median, Days) ดังกราฟแสดงในภาพที่ 4 |
ลดเวลา | 11 | 2 | < 0.001 HR = 2.01 95% CI; 1.53 – 2.62 |
| Time from First Visit to First Treatment (Median, Days) ดังกราฟแสดงในภาพที่ 4 |
ลดเวลา | 57 | 14 | < 0.001 HR = 2.93 95% CI; 2.21 – 3.89 |
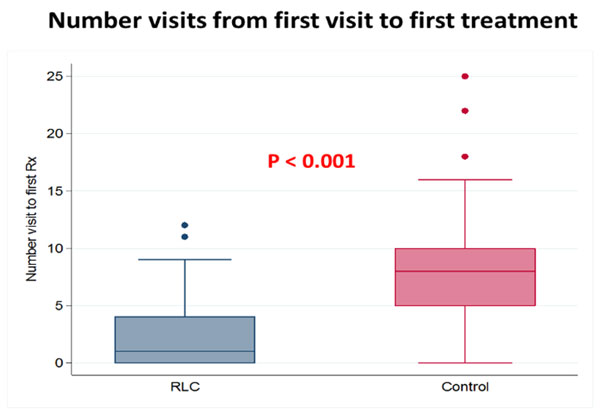
| Number Visits from First Visit to First Treatment (Mean +- SD, Days) ดังแสดงในภาพที่ 5 |
ลดจำนวน Visits | 7.98 ± 4.47 | 2.27 ± 2.70 | < 0.001 |
หมายเหตุ :
• Time from First Visit to First Intervention คือ เวลาตั้งแต่ที่มาโรงพยาบาลรามาธิบดี ที่เริ่มสงสัยว่าเป็นโรคมะเร็งปอด จนกระทั่งถึงเวลาที่ได้รับการตรวจประเมินด้วยวิธีใด ๆ เช่น การทำ Biopsy, Imaging Study, การนัดพบแพทย์, การเริ่มรักษา เทียบกันระหว่างก่อนและหลังมีการจัดตั้ง RLC
• Time from First Visit to First Treatment คือ เวลาตั้งแต่ที่มาโรงพยาบาลรามาธิบดี ที่เริ่มสงสัยว่าเป็นโรคมะเร็งปอด จนกระทั่งถึงเวลาที่เริ่มรักษา ด้วยการผ่าตัด การให้รังสีรักษา การให้ยาเคมีบำบัด หรือการให้ยาต้านเฉพาะจุด เทียบกันระหว่างก่อนและหลังมีการจัดตั้ง RLC
• Number Visits from First Visit to First Treatment คือ จำนวนครั้งที่มาโรงพยาบาลรามาธิบดี ตั้งแต่ที่เริ่มสงสัยว่าเป็นโรคมะเร็งปอด จนกระทั่งถึงเวลาที่เริ่มรักษา ด้วยการผ่าตัด การให้รังสีรักษา การให้ยาเคมีบำบัด หรือการให้ยาต้านเฉพาะจุด เทียบกันระหว่างก่อนและหลังมีการจัดตั้ง RLC
และนอกจากนี้ เมื่อนำมาวิเคราะห์ผลเพิ่มเติมถึงอัตราการอยู่รอดชีวิตของผู้ป่วยมะเร็งปอดที่ผ่าน RLC โมเดล พบว่าผู้ป่วยมีอัตราการอยู่รอดชีวิตที่ยืนยาวขึ้นอย่างมีนัยสำคัญทางสถิติ เมื่อเปรียบเทียบกับผู้ป่วยมะเร็งปอดที่ไม่ได้ผ่าน RLC โมเดล หรือผู้ป่วยมะเร็งปอดก่อนมีการจัดตั้ง RLC ดังแสดงในตารางที่ 4 และเมื่อแยกผู้ป่วยตามระยะของโรคคือ ระยะแรกเริ่ม (Stage 1 – 2 : ระยะที่รักษาหายจากการผ่าตัดเป็นหลัก) และระยะที่เป็นมากหรือระยะลุกลาม (Stage 3 – 4) ก็พบว่าผู้ป่วยมะเร็งปอดที่มีระยะของโรคเป็นระยะ 3 – 4 นั้น ถ้าผ่านกลไกการทำงานของ RLC โมเดล จะมี Overall Survival (OS) หรือความยืนยาวของชีวิตที่มากกว่าผู้ป่วยที่ไม่ได้ผ่าน RLC อย่างมีนัยสำคัญทางสถิติ ดังแสดงในภาพที่ 6 ส่วนในระยะแรกเริ่มนั้นขณะนี้ OS ยังไม่ต่างกันระหว่างสองกลุ่ม เนื่องจากเป็นระยะที่อัตราการรอดชีวิตสูงอยู่แล้ว และขณะนี้ระยะเวลาในการติดตามยังไม่มากพอ
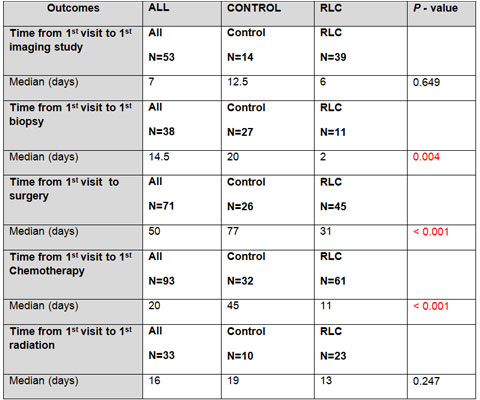
ตารางที่ 3 : แสดงตัวชี้วัดผลสำเร็จรอง ผลดำเนินโครงการ เปรียบเทียบระหว่างก่อนและหลังมีการจัดตั้ง RLC
| ตัวชี้วัด | ALL | CONTROL | RLC | P – Value |
| Time from 1st Visit to 1st Imaging Study | All N = 53 |
Control N = 14 |
RLC N = 39 |
|
| Median (Days) | 7 | 12.5 | 6 | 0.649 |
| Time from 1st Visit to 1st Biopsy | All N = 38 |
Control N = 27 |
RLC N = 11 |
|
| Median (Days) | 14.5 | 20 | 2 | 0.004 |
| Time from 1st Visit to Surgery | All N = 71 |
Control N = 26 |
RLC N = 45 |
|
| Median (Days) | 50 | 77 | 31 | < 0.001 |
| Time from 1st Visit to 1st Chemotherapy | All N = 93 |
Control N = 32 |
RLC N = 61 |
|
| Median (Days) | 20 | 45 | 11 | < 0.001 |
| Time from 1st Visit to 1st Radiation | All N = 33 |
Control N = 10 |
RLC N = 23 |
|
| Median (Days) | 16 | 19 | 13 | 0.247 |
ตารางที่ 4 : แสดงอัตราการรอดชีวิตที่ 5 ปี และ Overall Survival ของผู้ป่วยมะเร็งปอด เปรียบเทียบก่อนและหลังมีการจัดตั้ง RLC
| กลุ่มผู้ป่วย | 5 – Year OS Rate (%) | P – Value | mOS (Years) | P – Value |
| ก่อนจัดตั้ง RLC (Control) | 33.1 (22.5 – 44.0) | < 0.001 | 1.5 | < 0.001 |
| หลังจัดตั้ง RLC | 45.9 (23.1 – 66.1) | 4.7 |
บทเรียนที่ได้รับ : บรรลุวัตถุประสงค์การจัดตั้งกลุ่มในทุกแง่มุมทั้งในแง่การบริการ การตรวจรักษา การเรียนการสอน และการทำวิจัย และจะมีการดำเนินการต่อเนื่องไปตลอด และจะนำ RLC Model นี้ไปเผยแพร่กับสถาบันอื่น ๆ เพื่อทำให้พัฒนาการรักษาผู้ป่วยโรคมะเร็งปอด และมะเร็งชนิดอื่น ๆ ของประเทศไทยดีขึ้น และหากสามารถขยายผลให้เป็นนโยบายของประเทศในการรักษาโรคมะเร็งชนิดอื่น ๆ ด้วยจักทำให้เกิดประโยชน์มากขึ้นในการใช้โมเดลนี้ รวมทั้งหากใช้โมเดล จะทำให้มีการประหยัดค่าใช้จ่ายต่าง ๆ ที่เกิดขึ้นจากการรักษามะเร็งปอด ทั้งทางตรงและทางอ้อม ที่สำคัญทำให้คุณภาพชีวิต และอัตราการรอดของชีวิตในผู้ป่วยมะเร็งปอดยืนยาวขึ้น
โอกาสพัฒนาในครั้งต่อไป : นำ RLC Model นี้ไปเผยแพร่กับสถาบันอื่น ๆ เพื่อทำให้พัฒนาการรักษาผู้ป่วยโรคมะเร็งปอด และรวมถึงมะเร็งชนิดอื่น ๆ ของประเทศไทยดีขึ้น รวมทั้งปัจจุบันได้มีการทำวิจัยร่วมกันใน RLC เกี่ยวกับโรคมะเร็งปอดในหลายโครงการวิจัย และมีการจัดงานประชุมวิชาการเรื่องโรคมะเร็งปอดร่วมกัน ในวันที่ 8 กุมภาพันธ์ พ.ศ. 2561 ซึ่งประสบความสำเร็จอย่างมากมีผู้เข้าฟังเป็นจำนวนมาก
การนำไปใช้ประโยชน์ : นำมาใช้ในการรักษาโรคมะเร็งปอด และพัฒนาเป็นคลินิกเฉพาะทางโรคมะเร็งปอด
รางวัลที่ได้รับ :
• รางวัลผลงานวิจัยดีเด่นภูมิภาคเอเชีย ได้รับรางวัล The 5th Kobayashi Foundation Award จากประเทศญี่ปุ่น [16 มิถุนายน พ.ศ. 2561]
• รางวัลชนะเลิศ Best Abstract Award of The Year 2018 (Academic Center) จากราชวิทยาลัยอายุรแพทย์แห่งประเทศไทย [27 เมษายน พ.ศ. 2561]
• รางวัล Team Good Practice Award จากมหาวิทยาลัยมหิดล ปี 2018
• รางวัลชนะเลิศ งานพัฒนาคุณภาพ ปี 2017 จากคณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล
การติดต่อ :
ผศ.พญ.ธัญนันท์ เรืองเวทย์วัฒนา
หน่วยมะเร็งวิทยา ภาควิชาอายุรศาสตร์
คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล
+ 668 9856 5656, +66 2 201 1671 – 2
thanyanan.reu@mahidol.ac.th, treungwetwattana@gmail.com
{:}{:en}
Ramathibodi Lung Cancer Consortium Model
Ramathibodi Comprehensive Cancer Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University
Title :
Ramathibodi Lung Cancer Consortium Model
Researchers :
Asst.Prof.Dr.Thanyanan Reungwetwattana (Principal Investigator)
Ramathibodi Lung Cancer Consortium (RLC)
Background and Rationale :
Lung cancer is one of the most common and burden disease worldwide including Thailand. Its mortality is highest compared to the other cancers in Thailand. Numbers of lung cancer patient in our hospital (Ramathibodi Hospital) is higher year by year as shown in Figure 1.
Currently, the technologies for investigation, diagnosis, and treatment for lung cancer both chemotherapy and targeted therapy are very advance to improve the survival and quality of life for the patients. Once the patient is suspected to have lung cancer, then a lot of investigations will be subsequently performed with a lot of appointments to meet the sub-specialties involved in lung cancer field, for example, meeting with pulmonologist/x-ray interventionist for tissue biopsy in order to get the diagnosis and molecular testing, imaging studies will be done for staging disease, meeting with surgeon for planning surgery, and meeting with medical oncologist/radio-oncologist if chemotherapy/targeted therapy or radiation is needed for the treatment. All of these processes sometime take a long time to complete investigation before starting the treatment (Figure 2) which may affect the outcome of treatment including patient’s symptoms, survival, and quality of life.
Goals :
Our group (RLC; Ramathibodi Lung Cancer Consortium) was established on October 7, 2014, aims firstly to help the patients accessing all investigations and treatments faster by review, discussion, seeing the patient and planning the treatment together as the multidisciplinary team and patient-center with one-stop service system as shown in Figure 3. Secondly, our group aims to work on lung cancer research together to explore the new knowledge. Thirdly, we aims to update and educate patients and all personnel involved in lung cancer field including residents and fellows.

Method :
1.) We have arranged the RLC meeting every 1st and 3rd Tuesday of the month to review, discuss, and solve the problems for lung cancer patients since October 7, 2014. As of May 2017 (2.5 years), 236 new lung cancer patients were solved all problems by RLC team. We had 15 short lectures before starting the RLC meeting for updating and educating all personnel. We also had 12 RLC committee meetings at the 5th Tuesday of the month to discuss the activities in RLC and how to improve the quality of RLC.
2.) We collected and analyzed the data of lung cancer patient between 2 groups. The first group is the patient whom underwent RLC model (case = 200 cases) and the second group is controlled group which was the patient whom diagnosed and treated before establishing RLC team (control = 81 cases). Our primary endpoint is time from first visit to first treatment [time from suspected to have lung cancer to time of first treatment (surgery, chemotherapy, or radiation)]. Secondary endpoints are time from first visit to first intervention (time from suspected to have lung cancer to time of first biopsy, imaging study, or treatment), number visits from first visit to first treatment. We also did subgroups analysis for time from first visit to first biopsy, time from first visit to first surgery, time from first visit to chemotherapy, and time from first visit to radiation.
Results :
Table 1 : Primary and secondary outcomes compared between before and after RLC establishment
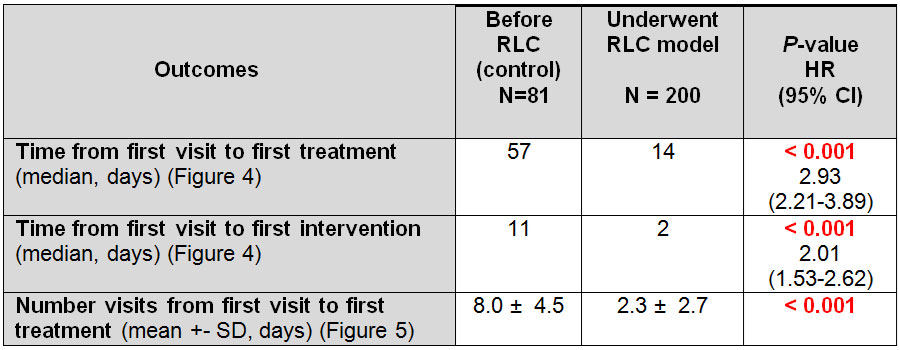
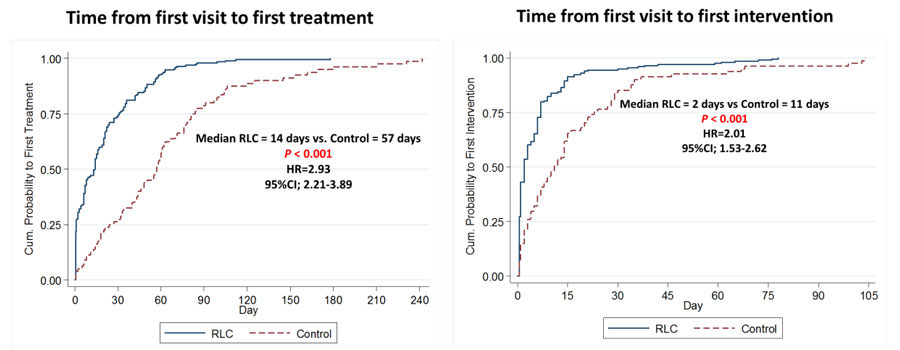
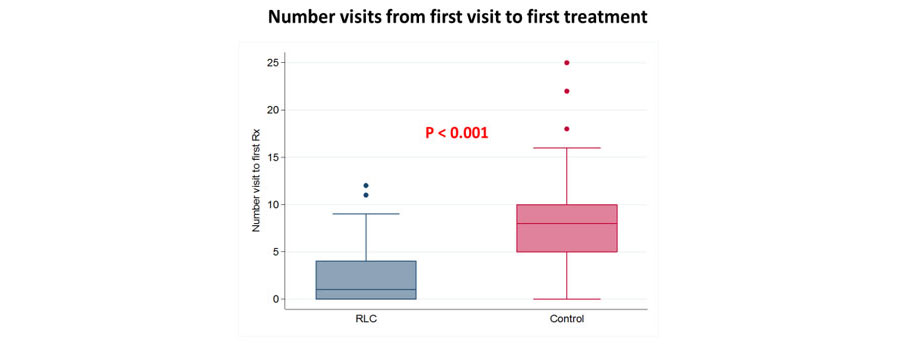
Table 2 : Subgroup analyses compared between before and after RLC establishment
Median time from first visit to first treatment was significantly decreased in RLC group (14 days) compared to 57 days in control group with hazard ratio of 2.93 (95% CI; 2.21-3.89, P<0.001) (Table 1, Figure 4). Median time from first visit to first intervention was also significantly decreased in RLC group (2 days) compared to 11 days in control group with hazard ratio of 2.01 (95% CI; 1.53-2.62, P<0.001) (Table 1, Figure 4). Median number of hospital visits was significantly lower in RLC group (2 visits) compared to control group (8 visits) (Table 1, Figure 5).
The subgroup analyses were performed and the results were significantly decreased in all secondary outcomes except time from first visit to first imaging study and first radiation because both of time from first visit to these 2 modalities was low in the existing process (Table 2).
Figure 6 and Table 3 : Overall survival compared between before and after RLC establishment
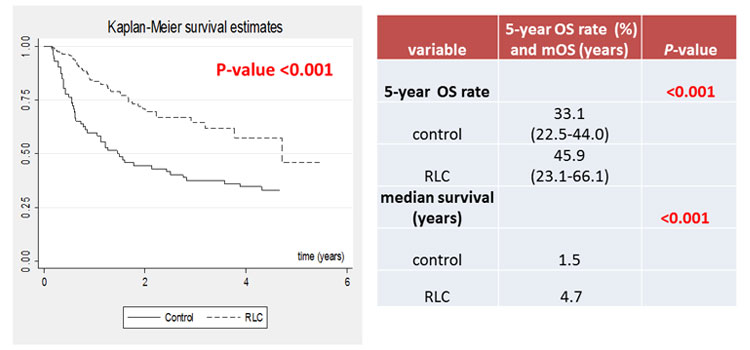
We performed survival analysis as shown in Figure 6 and Table 3. The new lung cancer patients whom underwent RLC model had significantly better median overall survival (OS) and 5-year OS rate, especially in stage 3 and 4 disease (mOS = 2.9 vs 0.6 years, HR=0.32 (95% CI; 0.2-0.5, P<0.001) as shown in figure 7.
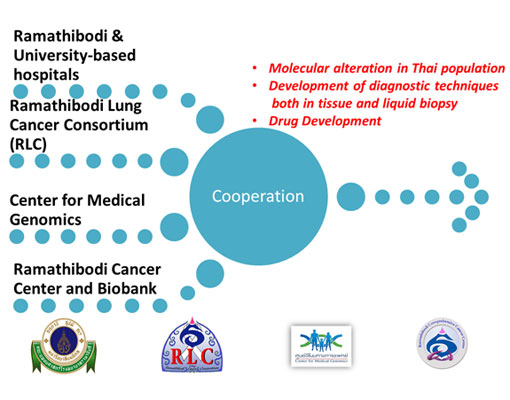
Furthermore, to serve our second aim which is performing the lung cancer research together, currently we have got the government grant to explore the molecular alteration in Thai lung cancer patients and develop in-house molecular testing both in tissue and plasma (Figure 8).
Finally, regarding our last aim about the education, we will arrange the first multidisciplinary team conference in February 2018 (The First Ramathibodi Lung Cancer Consortium: Optimizing treatment 2018). We will have renowned speakers as Professor Alex Adjei, Professor Tony Mok, and Associate Professor Julian Molina joining our conference and being our honor speakers as shown in Figure 9.

Conclusion :
We have established RLC for totally 3 years. We accomplish our 3 goals. First goal, our patient could access treatment and investigation in short period of time and leading to have the better survival as shown in results part. Second goal, we have the ongoing lung cancer research which we work together to explore and establish the new knowledge in lung cancer field. Third goal, we will arrange the academic conference in February 8, 2017 as mentioned previously. RLC model is the very useful model for lung cancer patients which translate to significantly better survival and all outcomes and RLC model is also the whole picture model for lung cancer treatment for both patients and personnel from BENCH to BEDSIDE.
“Working as Multidisciplinary Team is the Utmost Importance for Lung Cancer Treatment.”
Key Contact Person :
Asst.Prof.Dr.Thanyanan Reungwetwattana
Oncology, Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University
+ 668 9856 5656, +66 2 201 1671 – 2
thanyanan.reu@mahidol.ac.th, treungwetwattana@gmail.com
{:}